*Stratified by serum β2-microglobulin (< 2.5 vs ≥ 2.5 mg/L), prior bortezomib (yes vs no), and prior lenalidomide (yes vs no).
†If a patient progressed during any bortezomib-containing regimen,
he/she was eligible to enroll if the progression date occurred after discontinuation of bortezomib.
‡NYHA classification of heart failure III is defined as: Marked limitation of physical activity. Comfortable at rest.
Less than ordinary activity causes fatigue, palpitation, or dyspnea (shortness of breath).
IV is defined as: Unable to carry out any physical activity without discomfort. Symptoms of heart failure at rest.
If any physical activity is undertaken, discomfort increases.
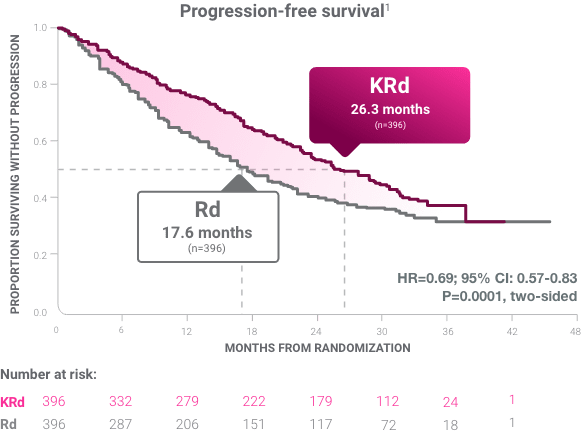
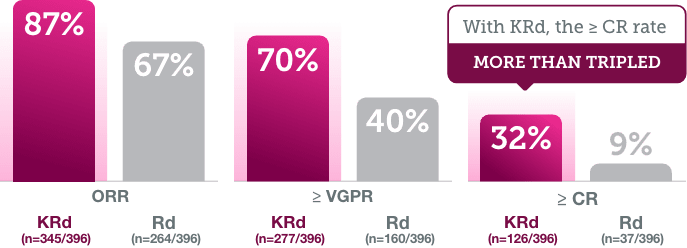
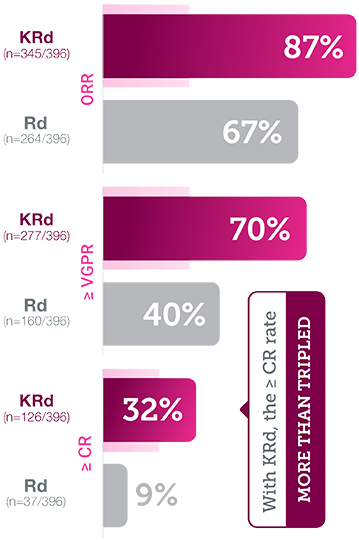
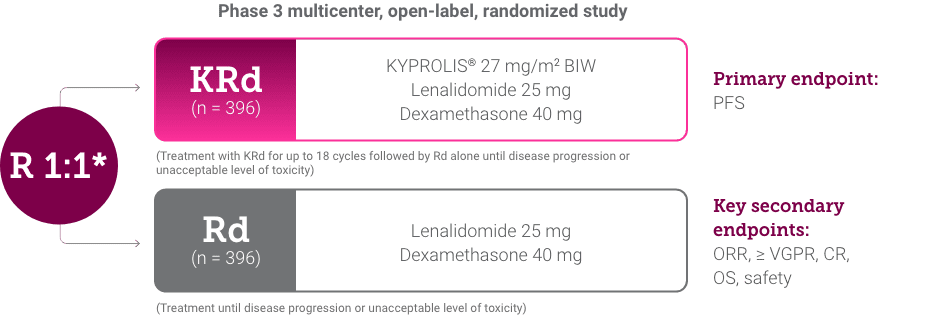
KRd = carfilzomib + lenalidomide + dexamethasone; Rd = lenalidomide + dexamethasone;
R = randomization; mg/m2 = milligrams per meter squared body surface area;
BIW = twice a week; mg = milligram; PFS = progression-free survival;
ORR = overall response rate; VGPR = very good partial response; MRD = minimal residual disease;
CR = complete response; OS = overall survival; MM = multiple myeloma; NYHA = New York Heart Association;
MR = median response; PD = progressive disease; Tx = treatment.