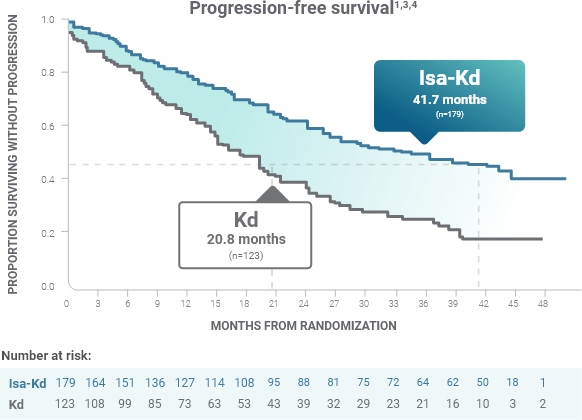
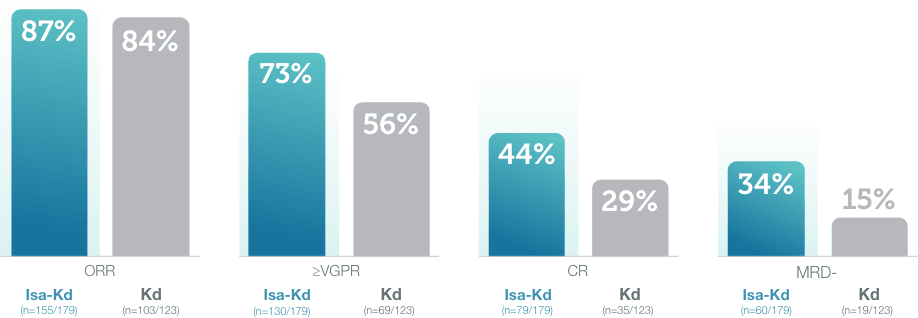
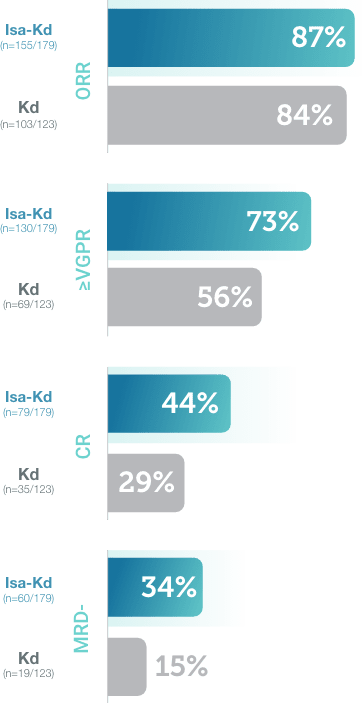
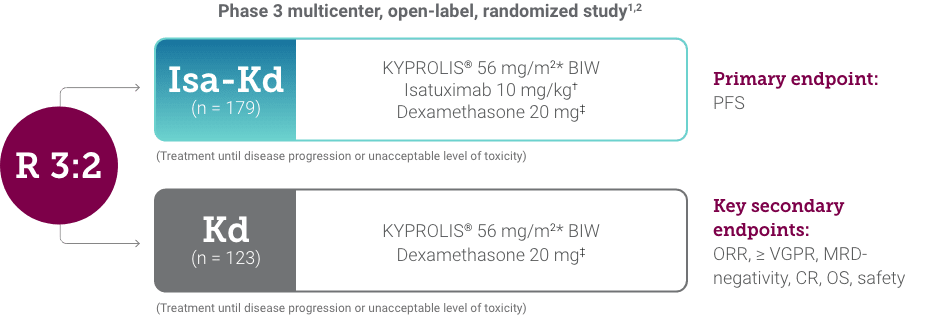
References: 1. SARCLISA® (isatuximab-irfc) prescribing information. Bridgewater, NJ: sanofi-aventis U.S. LLC. 2. Moreau P, Dimopoulos MA, Mikhael J, et al. Isatuximab, carfilzomib, and dexamethasone in relapsed multiple myeloma (IKEMA): a multicentre, open-label, randomised phase 3 trial. Lancet. 2021;397(10292):2361-2371. 3. Martin, T, Dimopoulos, M a C, et al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized Phase 3 study. Blood Cancer J. 2023;13:72:1,9. 4. Moreau P, Dimopoulos M-A, Mikhael J, et al. Updated progression-free survival and depth of response in IKEMA, a randomized phase III trial of isatuximab, carfilzomib and dexamethasone (Isa-Kd) vs Kd in relapsed multiple myeloma. Presented at the ESMO Virtual Plenary, University Hospital Hôtel-Dieu, Nantes, France. May 19-20, 2022. 5. KYPROLIS® (carfilzomib) prescribing information, Onyx Pharmaceuticals Inc., an Amgen Inc. subsidiary.