*Patient stratification included prior proteasome inhibitor therapy (either bortezomib or carfilzomib,
or no prior therapy); prior lines of therapy (1 vs 2 or 3);
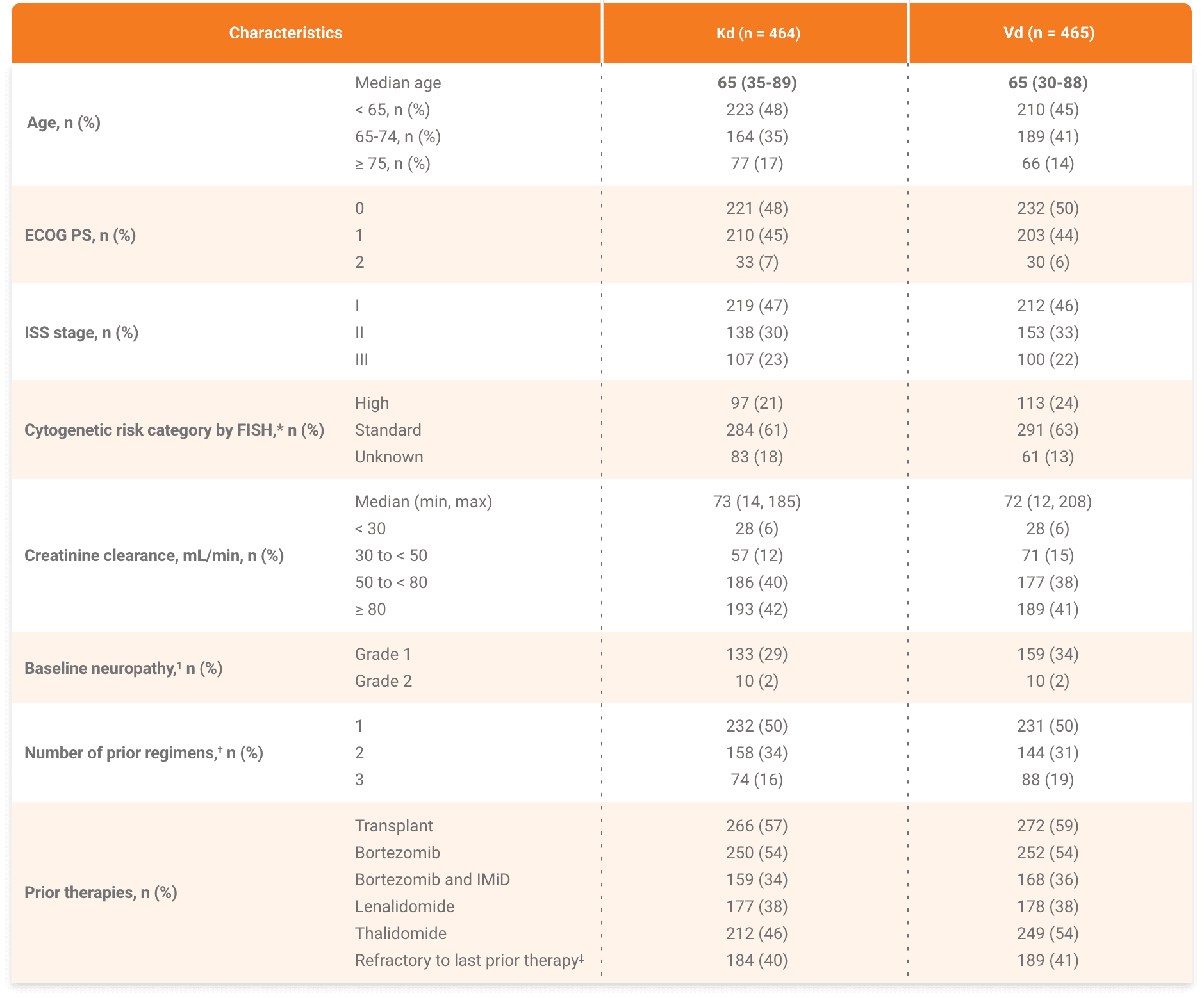
International Staging System stage (1 vs 2 or 3); and planned route of bortezomib administration,
if randomized to the bortezomib group (intravenous vs subcutaneous).
†NYHA classification of heart failure III is defined as: Marked limitation of physical activity.
Comfortable at rest. Less than ordinary activity causes fatigue, palpitation, or dyspnea (shortness of breath).
IV is defined as: Unable to carry out any physical activity without discomfort. Symptoms of heart failure at rest.
If any physical activity is undertaken, discomfort increases.
BIW, twice a week; CrCI, creatinine clearance; DoR, depth of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; Kd, carfilzomib and dexamethasone; LVEF, left ventricular ejection fraction; MM, multiple myeloma; NYHA, New York Heart Association; ORR, overall response rate; OS, overall survival;
PFS, progression-free survival; PI, proteasome inhibitor; PR, partial response; R, randomization; Vd, bortezomib and dexamethasone.